- Breast
- Partial Breast Reconstruction
Partial Breast
Reconstruction
The need for breast reconstruction
Breast cancer is a common condition among women. Almost one in seven women develops a tumor in one or both breasts during her life with an increase in incidence in the last decades. This rise in incidence might be due to longer life expectancy, but also because of better,
earlier, and larger cancer screening programs in Belgium and abroad. Early tumor detection and more aggressive treatment of breast cancer have fortunately resulted in a reduction of breast cancer-related mortality.
There are various treatments to fight breast cancer. For some women, it is sufficient to remove the tumor and some healthy tissue around it (tumorectomy or segmentectomy). This is referred to as breast- conserving surgery, as most of the healthy breast tissue is preserved.
Usually, these patients also receive additional treatment with local radiation therapy after the surgery to reduce the likelihood of the tumor to return.
For other women, there is no other option than to take away the complete breast (mastectomy). Additional radiotherapy or chemotherapy before or after the surgery may be indicated, depending on the type of breast tumor.
Not every woman reacts in the same way after a mastectomy. Some prefer to have the breast reconstruction to be performed as soon as possible, while others choose to wear an external prosthesis for a while. Some even prefer to do nothing.
It is a personal choice that you must make for yourself. But to make that choice, it may help if you know all the different types of treatment and reconstructive options.
Classic mastectomy : The breast gland is removed together with the nipple-areola complex and most of the breast skin resulting in a horizontal or oblique scar on the chest wall.
Skin-sparing mastectomy: The breast gland is removed together with the nipple-areola complex, but most of the breast skin will be spared, resulting in fewer and shorter scars.
Nipple-sparing mastectomy: The breast gland is removed but the nipple-areola complex and most of the breast skin are spared, giving the best aesthetic result. It is indicated in risk-reducing mastectomy (patients with a specific gene mutation that increases the risk of developing breast cancer throughout their life) or in selected cases where a small tumor is diagnosed at a distance from the nipple.
A breast reconstruction does not have any influence on the course of the disease. It has, in other words, no negative impact on the breast cancer treatment or its evolution. But it will often provide a better quality of life for the patient. In some cases, we can perform a breast reconstruction immediately after the tumor has been removed. This is called a primary or concurrent breast reconstruction and happens during the same surgery as the mastectomy. In other cases, it may be preferable to wait until any additional treatment (radio- and/or chemotherapy) has been finished. In that case, it is called a secondary or delayed breast reconstruction.
Both reconstructions have their advantages and disadvantages. We have listed them here for you:
Primary reconstruction
Advantages
- Two operations in one time with one recovery period
- Psychological advantage as the breast is immediately reconstructed The aesthetic result is usually better
- Improved wound healing
Disadvantages
- Radiation can cause a varying degree of stiffness and hardness to the reconstructed breast
Secondary reconstruction
Advantages
- Less stressful for the patient as all necessary treatments have been finished
- No influence of the radiotherapy on the reconstructed breast
Disadvantages
- Wound healing can sometimes be more difficult if radiotherapy was given, as this may affect the blood supply to the skin
- More skin should be replaced which might make a patch-effect, as a part of the skin may need to be removed if it is damaged by the radiotherapy
If there is no additional treatment necessary, a primary breast reconstruction is usually advised as it combines both procedures with only one recovery period. If there is any additional treatment necessary (radiotherapy or chemotherapy), we may prefer to opt for a secondary reconstruction and place a temporary breast implant (tissue expander) under the breast skin to maintain the breast cavity and skin envelope and facilitate the breast reconstruction afterward. This will be discussed in detail during the consultation.
There are various techniques to perform a breast reconstruction, but not every method suits every woman. At Ogeeplast Clinic, we find and suggest a suitable technique depending on a set of variables:
- Age
- Body morphology
- Breast form and volume
- Any (and all) previous operations
- Type of surgery to the breast (tumorectomy vs mastectomy) Possible treatment after the oncological surgery
- Your personal preference
Each technique has its advantages and disadvantages. With our vast experience in breast reconstruction, we take all factors into consideration and bring the various options to the table.
The different techniques
As previously mentioned, there are several techniques for breast reconstruction and several factors play a role in choosing the best technique for you.
Partial breast reconstruction
If the breast surgeon did not perform a complete breast amputation (in the case of breast-conserving surgery), several techniques for partial breast reconstruction exist :
- Reconstruction with a local tissue flap
- Breast reshaping/remodeling
- Reconstruction with pedicled flap
- Reconstruction with a free tissue flap
The best option will depend on the size of the removed tissue and the size of your breast. During the consultation, your breasts will be examined and a surgical plan will be suggested.
Total breast reconstruction
If a complete breast amputation (mastectomy) has or will be performed, then a total breast reconstruction will be planned. A total breast reconstruction may be done with your body tissue or with a breast implant. For both of these categories, different techniques are possible.
- Breast implant
- Silicone-filled breast implant Tissue expander
Own body tissue
- DIEP/SIEA flap or belly flap
- SGAP flap or buttock flap
- LAP flap or love-handle flap
- PAP flap or posterior thigh flap
- TMG/TUG flap or median thigh flap Fat
- transfer through lipofilling
PARTIAL BREAST RECONSTRUCTION
If breast-conserving surgery is possible through a tumorectomy or segmentectomy, then only a part of the breast needs to be reconstructed to restore the breast shape and volume. Depending on the size of the resected tissues and the overall size of the breast, one of the following procedures will be the best choice for you:
A local tissue or glandular flap from the breast itself or the tissue adjacent to the breast can be used to fill up the resulting defect after tumor removal. If adjacent tissue is used, you have to take an additional scar into account
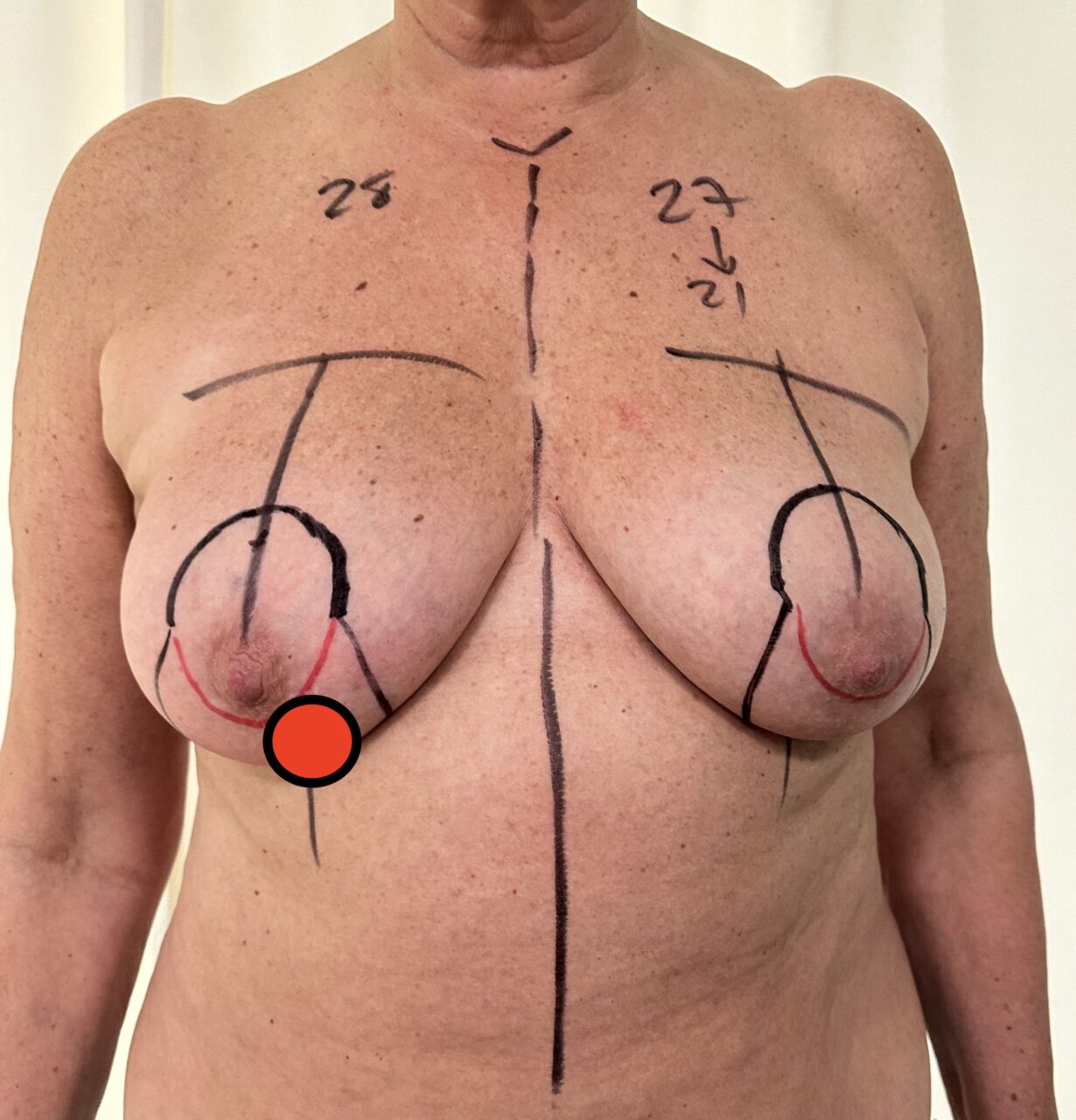
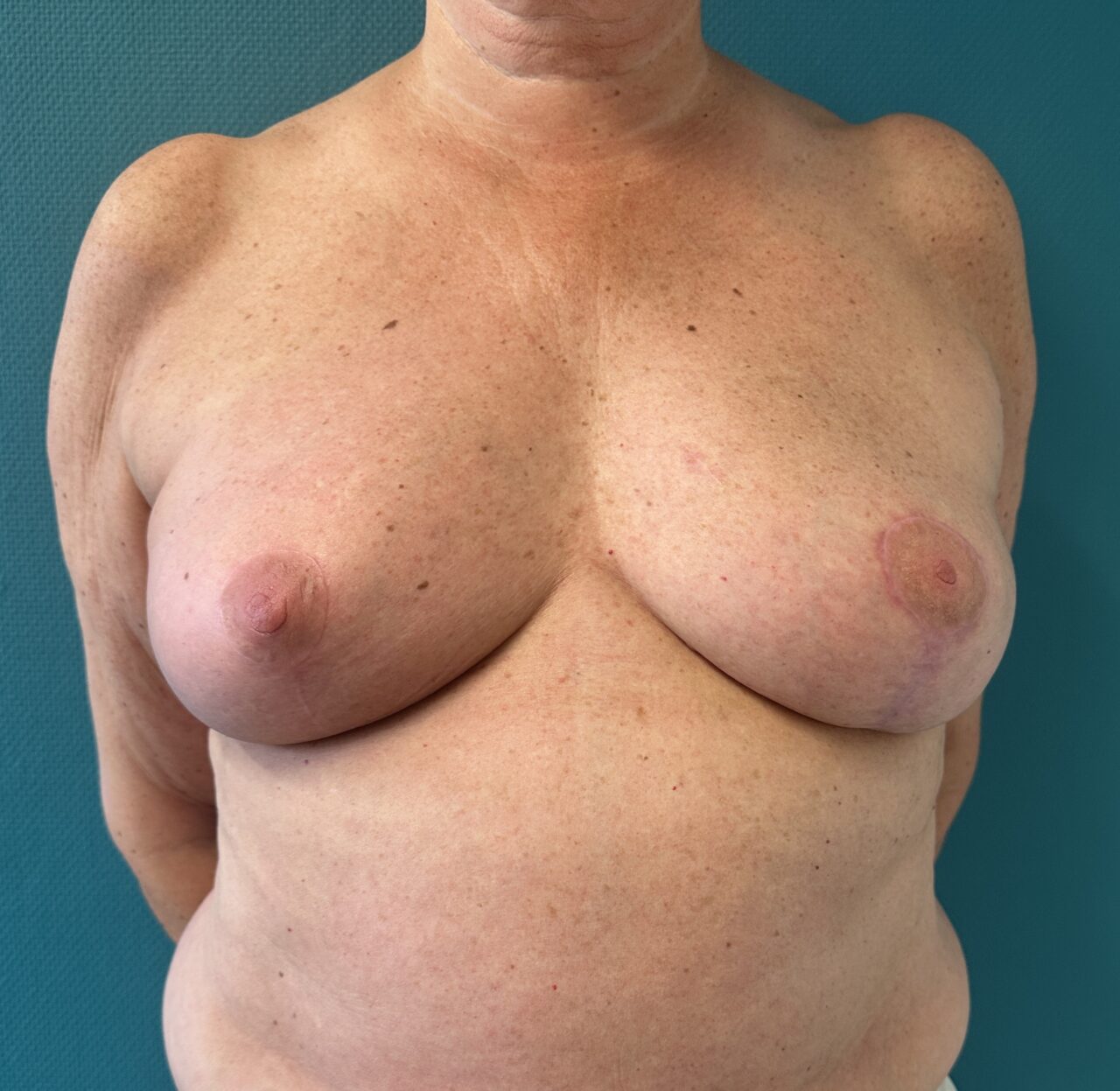
If you have a large breast volume and the amount of removed breast tissue is less than 30% of the total volume, a tumorectomy combined with a breast reduction is a very elegant procedure to both remove the breast tumor and reduce the overall breast size to give you smaller,
rounder breasts with natural shape and symmetry. The remaining tissue of the breast can be used to create a new smaller breast with natural proportions. By placing healthy tissue at the location of the previous breast tumor, your breast shape is also better preserved and protected during the radiotherapy.
This technique of breast reshaping is also possible if you had a previous tumorectomy without breast reconstruction but suffer from a deformed breast after the radiotherapy.
The scars that will remain after this procedure are located in the same place as a classic breast reduction, namely around the nipple, down over the lower pole of the breast, and along the infra-mammary fold.
The contralateral breast is usually also lifted and reduced, to create better symmetry.
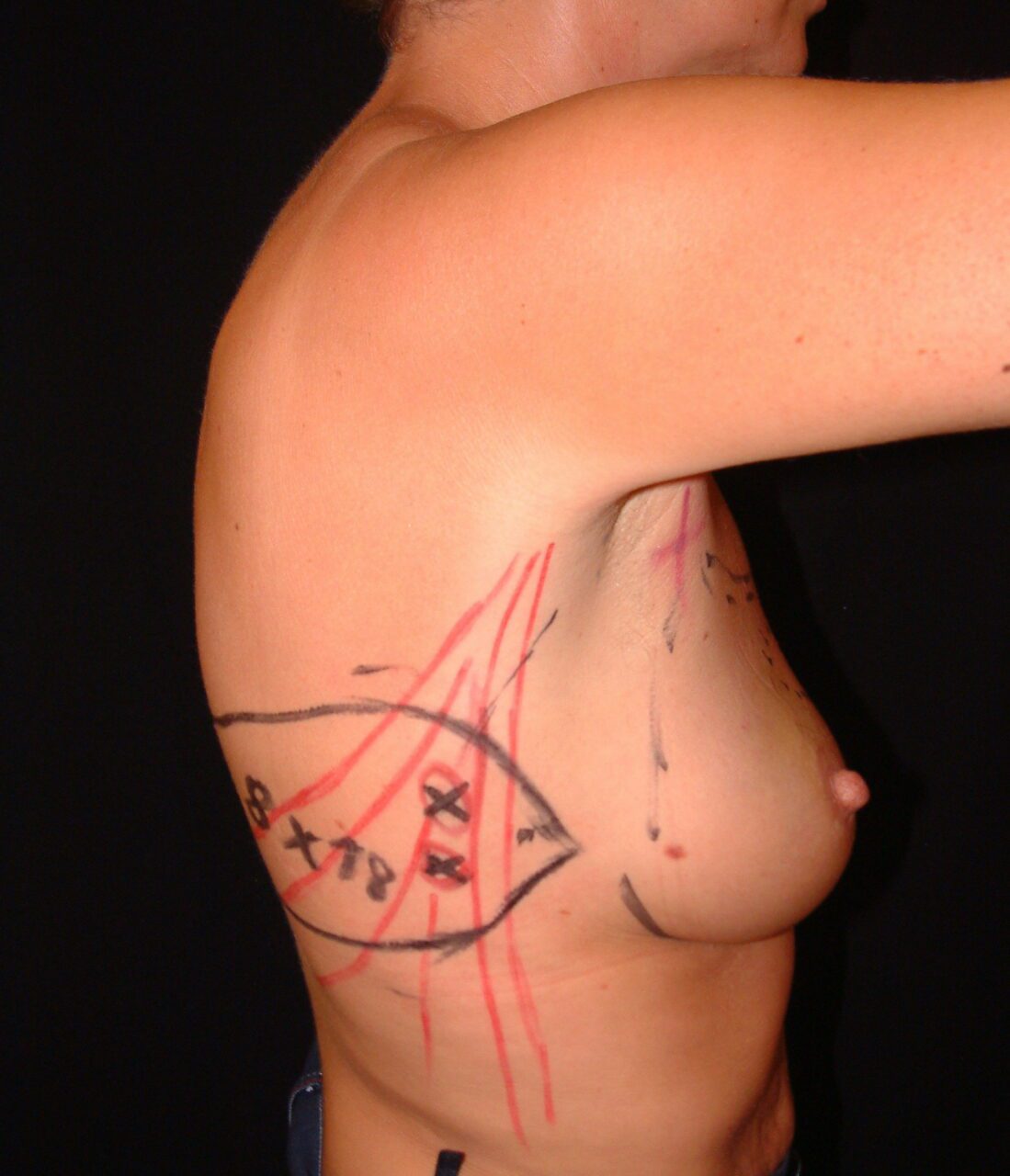
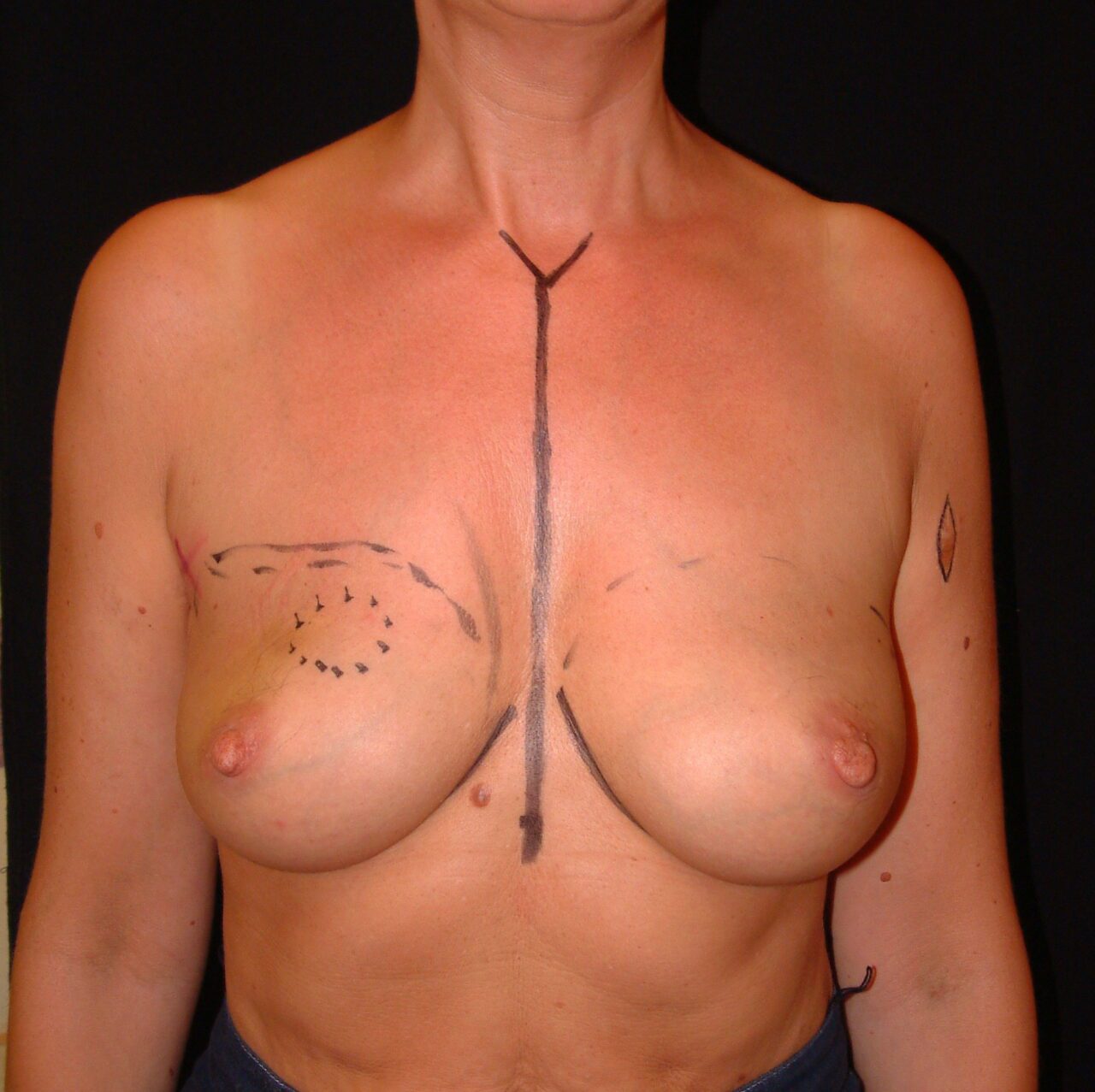
If you have relatively small breasts, there may not be enough healthy breast tissue left to reshape the breast after tumor removal. In that case, we can harvest additional tissue from a different part of your body, right next to your breast. This technique has been widely presented by Prof.
Hamdi all over the world. Two possible tissue flaps are commonly available.
For a reconstruction with a pedicled latissimus dorsi flap, we can use the large muscle of the back on the same side as the operated breast.
Via the armpit, the muscle flap is brought around the chest to the anterior side to fill the defect. Although this gives a sufficient amount of volume to reshape a natural-looking breast, a downside of this procedure is that one of the major muscles of the body is sacrificed. This will not impact your daily activities, but may not be a good option in very sporty women (for example rock climbers or athletes)
A second available tissue flap is the thoracodorsal artery perforator flap, located on the lateral chest wall. During this procedure, we only take the skin and fat from the lateral and posterior chest wall to fill the chest. The back muscle thus remains untouched, but the flap has a smaller volume.
Which technique is best for you depends on the size of the removed tissue and your body morphology. Both techniques involve an additional scar on the back which can be oriented diagonally upwards to the spine, along the lines of the skin folds or along the bra line.
When more than 30% of the breast tissue has to be removed, a total removal of the breast is sometimes indicated and therefore a mastectomy will be done. The reconstructive techniques are then the same as the ones applicable after a mastectomy (see below).